This virus is devious to say the least:
Young and middle-aged people, barely sick with covid-19, are dying from strokes
Doctors sound alarm about patients in their 30s and 40s left debilitated or dead. Some didn’t even know they were infected.
https://www.washingtonpost.com/health/2 ... -patients/
Wuhan Coronavirus Resource Thread
Re: Wuhan Coronavirus Resource Thread
China needs to be bloody held responsible for their irresponsible tinkering with science and utterly shameless attempt to cover it up. Fck I hope there are sanctions on them. Yes, I know its a double edged sword that can be used against us by releasing a virus/bioweapon here and then pretending we are equally at fault, but the PRC Govt needs to pay a price for the lives they have ruined. Ba$tards.
Re: Wuhan Coronavirus Resource Thread
LOL. Link? I believe Primus talking about the desi/NRI community in the US. Yes, I can say hygiene level among Indians here are higher than goras. At the very least, we do not wear our outside shoes in our house! Goras walking their dogs, stepping on places where other goras had walked their dogs and then tramping around home in the same shoes, are far more likely to have trace amounts of fecal matter in their household.Raveen wrote:Is that why there are trace amounts of fecal matter on every Indian Rupee note?Primus wrote:. We are as a culture more conscious of personal hygiene etc though
Re: Wuhan Coronavirus Resource Thread
I would add WHO also to that.Karan M wrote:China needs to be bloody held responsible . .. .
Re: Wuhan Coronavirus Resource Thread
WHO might be dead. But don't hold your breath for Cheen. Chances are increasing they'll ride this out and even if the world turns against them post-Wuhan.SSridhar wrote:I would add WHO also to that.Karan M wrote:China needs to be bloody held responsible . .. .
As far as retail for MNCs are concerned, Cheen sales are returning to normal pretty quickly. This is happening while they've been cut off from the world for close to three months now.
https://footwearnews.com/2020/business/ ... 202971578/
With the world de-globalizing, the countries and regions with the biggest internal markets will make out the best. They have THE biggest market.
Re: Wuhan Coronavirus Resource Thread
I agree. But who will bell the cat? Once the China virus is brought under control, the West may again follow the path of the least resistance. Another decade or two of business as usual will make Sugarland's position unassailable.Karan M wrote:China needs to be bloody held responsible for their irresponsible tinkering with science and utterly shameless attempt to cover it up. Fck I hope there are sanctions on them. Yes, I know its a double edged sword that can be used against us by releasing a virus/bioweapon here and then pretending we are equally at fault, but the PRC Govt needs to pay a price for the lives they have ruined. Ba$tards.
Gautam
Re: Wuhan Coronavirus Resource Thread
If China is open, why are the Injection die toolmakers and prototype makers there delaying the consignments?chola wrote:WHO might be dead. But don't hold your breath for Cheen. Chances are increasing they'll ride this out and even if the world turns against them post-Wuhan.SSridhar wrote: I would add WHO also to that.
As far as retail for MNCs are concerned, Cheen sales are returning to normal pretty quickly. This is happening while they've been cut off from the world for close to three months now.
https://footwearnews.com/2020/business/ ... 202971578/
With the world de-globalizing, the countries and regions with the biggest internal markets will make out the best. They have THE biggest market.
South Korean , Taiwanese and the Japanese are ready to ship.
Re: Wuhan Coronavirus Resource Thread
They aren't open. Not internationally. In fact, they've closed themselves off further by restricting international flights further to avoid a second wave. The MNCs are pressing to get boots on the ground there but can't.Krita wrote:If China is open, why are the Injection die toolmakers and prototype makers there delaying the consignments?chola wrote:
WHO might be dead. But don't hold your breath for Cheen. Chances are increasing they'll ride this out and even if the world turns against them post-Wuhan.
As far as retail for MNCs are concerned, Cheen sales are returning to normal pretty quickly. This is happening while they've been cut off from the world for close to three months now.
https://footwearnews.com/2020/business/ ... 202971578/
With the world de-globalizing, the countries and regions with the biggest internal markets will make out the best. They have THE biggest market.
South Korean , Taiwanese and the Japanese are ready to ship.
But their economy is returning to normal. MNCs with operations there are seeing spikes. Corporate boards are already predicting that May 1st there would a massive day for retail and travel. Cheen is the ONLY good news these days on Wall Street.
Re: Wuhan Coronavirus Resource Thread
https://www.themoscowtimes.com/2020/04/ ... -24-a69117
Coronavirus in Russia: The Latest News | April 25
As the new coronavirus that has killed more than 190,000 people worldwide continues to spread, Russia has stepped up its measures to slow the pandemic's spread within its borders.
There have been 68,622 cases of coronavirus infections reported in Russia so far and 615 deaths.
April 25: 3 things you need to know today
Russia confirmed 5,849 new coronavirus infections Friday, bringing the country’s official number of cases to 68,622. Overall, 615 people have been killed by the virus.
Moscow authorities will not ease the city's self-isolation orders during the May holidays which include Labor Day and Victory Day, the mayor's office said. Meanwhile, the head of Russia’s consumer health watchdog argued self-isolation should be extended by at least another two weeks, until the middle of May.
Moscow Mayor Sergei Sobyanin said he has asked Russia's Health Ministry and Education Ministry to prepare fourth- and fifth-year medical students to help treat coronavirus patients.
.....
Gautam
Coronavirus in Russia: The Latest News | April 25
As the new coronavirus that has killed more than 190,000 people worldwide continues to spread, Russia has stepped up its measures to slow the pandemic's spread within its borders.
There have been 68,622 cases of coronavirus infections reported in Russia so far and 615 deaths.
April 25: 3 things you need to know today
Russia confirmed 5,849 new coronavirus infections Friday, bringing the country’s official number of cases to 68,622. Overall, 615 people have been killed by the virus.
Moscow authorities will not ease the city's self-isolation orders during the May holidays which include Labor Day and Victory Day, the mayor's office said. Meanwhile, the head of Russia’s consumer health watchdog argued self-isolation should be extended by at least another two weeks, until the middle of May.
Moscow Mayor Sergei Sobyanin said he has asked Russia's Health Ministry and Education Ministry to prepare fourth- and fifth-year medical students to help treat coronavirus patients.
.....
Gautam
Re: Wuhan Coronavirus Resource Thread
The tale of the dragon & the Guinea pig.
China to Pakistan: We have a vaccine.
We don’t know if it works.
You try it on yourself.
If you don’t die, we’ll sell it to you.
Pakistan: This is “a great thing for Pakistan,” we’ll get vaccines on “high-priority.”
https://twitter.com/wionews/status/1253397206960201729
Re: Wuhan Coronavirus Resource Thread
811 new #COVID19 cases and 22 deaths have been reported in the state today, taking the total number of positive cases to 7628 and death toll to 323: Maharashtra Health Department
Re: Wuhan Coronavirus Resource Thread
on cue: the lancet weighs in
the bleddy britshits who right royally effed up their chinese virus response using "herd immunity" as the best way forward as well as skewering themselves with a badly timed and deceitfully conceived brexit are back to advising the brown skinned natives once again while their own tattered underpants have been bunched around their whitey ankles for the longest time now.
somehow, they don't seem to like this eternal sunset that they find themselves in these days.
also, the britshits are lucky indeed because as long as there are publications like this lancet, they will never run short of toilet paper.
COVID-19 Pandemic used to fan anti-Muslim sentiment in India, says Lancet
the bleddy britshits who right royally effed up their chinese virus response using "herd immunity" as the best way forward as well as skewering themselves with a badly timed and deceitfully conceived brexit are back to advising the brown skinned natives once again while their own tattered underpants have been bunched around their whitey ankles for the longest time now.
somehow, they don't seem to like this eternal sunset that they find themselves in these days.
also, the britshits are lucky indeed because as long as there are publications like this lancet, they will never run short of toilet paper.
COVID-19 Pandemic used to fan anti-Muslim sentiment in India, says Lancet
The editorial in one of the world’s leading medical journal 'The Lancet' has strongly criticized the massive nationwide lockdown in India--adopted in order to contain COVID-19 pandemic--suggesting that it has caused hardships, hunger and misery to millions of the most vulnerable people in the country.
Citing the example of the misinformation campaign run around Tablighi Jamaat, the piece also said that the pandemic has been used to “fan anti-Muslim sentiment” adding that one threat to the COVID-19 response in India is the spread of misinformation driven by fear, stigma, and blame.
Pointing out at the recent mass exodus of migrant workers during the lockdown and concerns rising about starvation among people who work in the informal economy, the Lancet said, “The government’s sudden enforcement of the lockdown seemed hastily prepared and immediately disadvantaged already vulnerable populations".
The Lancet highlighted that government’s efforts to provide financial support and a measure of food security to ease these pressures will be insufficient to meet demand, but better planning and communication could have helped avert this crisis.
Similarly, non-COVID 19 health services have been disrupted as India’s public health-care system is chronically underfunded --at just 1·28 per cent of GDP, leaving primary care weak--it noted
The editorial however also pointed out that in India’s favour is its young population (65 per cent aged below 35 years) and, to date, the country has seen a less severe outbreak than was feared, and the lockdown could be already having the desired effect of flattening the curve.
Re: Wuhan Coronavirus Resource Thread
just in time when ramzan is starting.sajo wrote:It seems the lockdown has been relaxed.
https://twitter.com/PIBHomeAffairs/stat ... 94176?s=09
#COVID19 update
All registered shops regd under Shops & Establishment Act of respective States/ UTs, including shops in residential complexes, neighborhood & standalone shops exempted from #lockdown restrictions.
Prohibited: Shops in single & multi brand malls https://t.co/NNz9abgWdAI expect traffic jams tomorrow.Market complexes, except those within the limits of municipal corporations and municipalities, are allowed to open.
Mandatory: 50% strength of workers, wearing of masks & observing #SocialDistancing
Relaxations not applicable in #Hotspots/containment zones
Isn't the timing suspicious/convenient
Re: Wuhan Coronavirus Resource Thread
[
All our experience has so far pointed out clearly that QuranoVirus is more virulent and deadlier than Coronavirus. Why should I risk my frontline police and health care worker to the triple dose of Quranovirus (stone pelting, rioting), #thookers and #thooblighis and Coronavirus?
As it is QuranoVirus is difficult to control. Add in the steroid of Ramzan and their daily "rozas" and "iftars" and trying to control the crowd at night! If this isn't a nightmare then what it is? Here is one example: https://twitter.com/zayen/status/1254054023767789569
It is known that as any epidemic spreads, it actually gets less virulent. All the strains that kill the host kills itself. Virus is a parasite and its best chances to live and evolve is for it to ensure that its host does not die. For example the rhinovirus that causes cold. It rarely kills its host. Some children get different and as many as dozens of infections in a year.
If the special community or single source want to be the first vectors of this disease and bear the brunt. So be it. Anyway the #Thooblighis turned the knife in Bharat's back https://twitter.com/ShamikaRavi/status/ ... 16/photo/1
The silver lining on the #Thooblighis going around as vectors is that they revealed their own network and reach. And the virus is taking them down. Imagine the outcry from the commie-left-red-rags if the government had gone after say 2000 Jamaatis in a nationwide operation in normal times? Imagine if 20 of those #Thookers would have died because of their underlying medical conditions naturally? That would have been an international outcry.
On WuhanVirus, some states are doing better than others: . So why those states and districts that are doing well be penalized?
. So why those states and districts that are doing well be penalized?
Also the death rate is low, it is coming to @3 per 1000. When the disease was a big unknown immediate lockdowns and safety was a necessary step and hopefully gain control over it. Now economy also matters. Of course, wholesale opening of economy is out of question. So what can one do? How can one open up economy in stages?
Raita wing who complain that Ram navami and Parshuram Jayanti is not publicly celebrated but Ramzan is, miss the point by a wide margin. If the other community want to take the risk by participating in religious congregations, let them. Once sickness and death knocks at their doors, they will react with bewilderment and realize that their own Quranovirus is the causative factor. Hopefully tube lights will light up. Like it did in WB.
I think if I were an administrator, I would also start thinking of opening up the economy now and use the Ramzan as a test.chetak wrote: just in time when ramzan is starting.
Isn't the timing suspicious/convenient
All our experience has so far pointed out clearly that QuranoVirus is more virulent and deadlier than Coronavirus. Why should I risk my frontline police and health care worker to the triple dose of Quranovirus (stone pelting, rioting), #thookers and #thooblighis and Coronavirus?
As it is QuranoVirus is difficult to control. Add in the steroid of Ramzan and their daily "rozas" and "iftars" and trying to control the crowd at night! If this isn't a nightmare then what it is? Here is one example: https://twitter.com/zayen/status/1254054023767789569
It is known that as any epidemic spreads, it actually gets less virulent. All the strains that kill the host kills itself. Virus is a parasite and its best chances to live and evolve is for it to ensure that its host does not die. For example the rhinovirus that causes cold. It rarely kills its host. Some children get different and as many as dozens of infections in a year.
If the special community or single source want to be the first vectors of this disease and bear the brunt. So be it. Anyway the #Thooblighis turned the knife in Bharat's back https://twitter.com/ShamikaRavi/status/ ... 16/photo/1
The silver lining on the #Thooblighis going around as vectors is that they revealed their own network and reach. And the virus is taking them down. Imagine the outcry from the commie-left-red-rags if the government had gone after say 2000 Jamaatis in a nationwide operation in normal times? Imagine if 20 of those #Thookers would have died because of their underlying medical conditions naturally? That would have been an international outcry.
On WuhanVirus, some states are doing better than others:
. So why those states and districts that are doing well be penalized? Also the death rate is low, it is coming to @3 per 1000. When the disease was a big unknown immediate lockdowns and safety was a necessary step and hopefully gain control over it. Now economy also matters. Of course, wholesale opening of economy is out of question. So what can one do? How can one open up economy in stages?
Raita wing who complain that Ram navami and Parshuram Jayanti is not publicly celebrated but Ramzan is, miss the point by a wide margin. If the other community want to take the risk by participating in religious congregations, let them. Once sickness and death knocks at their doors, they will react with bewilderment and realize that their own Quranovirus is the causative factor. Hopefully tube lights will light up. Like it did in WB.
Re: Wuhan Coronavirus Resource Thread
This is what Trump was talking about, treatment developed by Cedars Sinai Hospital. Basically a UV light which is inserted down via the mouth. Now licensed to Aytu BioScience. It is claimed to kill all kinds of viruses including the coronavirus.srai wrote:Anything coming out of Trump is a “misquote”Karan M wrote:
You are kidding me. Are you sure this is not a misquote?
Don’t watch his briefings for any value other than for entertainment purposes. Constantly peddling rumors, lies and partisan extremism. No substance.
Cedars-Sinai-Developed ‘Healight' Medical Device Platform Technology Being Studied as a Potential First-in-Class COVID-19 Treatment
https://streamable.com/w7rpbn
Re: Wuhan Coronavirus Resource Thread
^^^
Well, the next day he was saying what he said was in sarcasm
Well, the next day he was saying what he said was in sarcasm
-
DrRatnadip
- BRFite
- Posts: 604
- Joined: 31 Dec 2016 00:40
Re: Wuhan Coronavirus Resource Thread
https://m.timesofindia.com/india/after- ... 384555.cms
- Many states want to extend lockdown beyond 3 may.. I think its direct reaction to sudden in increase in Covid positive cases.. I dont think it is good idea to increase general lockdown further.. We need to find ways to gradually exit from it before lockdown itself starts killing more than Covid..
- very large chunk of our population is very young and least likely to suffer from serious consequences of disease.. We need to find ways to use this to our advantage..
- Many states want to extend lockdown beyond 3 may.. I think its direct reaction to sudden in increase in Covid positive cases.. I dont think it is good idea to increase general lockdown further.. We need to find ways to gradually exit from it before lockdown itself starts killing more than Covid..
- very large chunk of our population is very young and least likely to suffer from serious consequences of disease.. We need to find ways to use this to our advantage..
-
Mort Walker
- BRF Oldie
- Posts: 10040
- Joined: 31 May 2004 11:31
- Location: The rings around Uranus.
Re: Wuhan Coronavirus Resource Thread
Are you sure?srai wrote:^^^
Well, the next day he was saying what he said was in sarcasm

Re: Wuhan Coronavirus Resource Thread
I've been watching Trump's daily briefings for a while since there is so little high quality real time entertainment these days. Its clear that he suffers from a lot of personality disorders that would earn epithets like jerk, idiot, maniac, toxic....
One of these disorders is the compulsive need to be seen as the smartest person in the room, all the time. So he restates, paraphrases what stuff he has been able to comprehend so that he can show off to you that "he got it!", and since he considers everyone else to be dumber that himself, he'll dumb it down and explain it for you.
Endless source of entertainment with sometimes disastrous consequences.
One of these disorders is the compulsive need to be seen as the smartest person in the room, all the time. So he restates, paraphrases what stuff he has been able to comprehend so that he can show off to you that "he got it!", and since he considers everyone else to be dumber that himself, he'll dumb it down and explain it for you.
Endless source of entertainment with sometimes disastrous consequences.
Re: Wuhan Coronavirus Resource Thread
What would you call the Indians who support morons like AOC, Killary and ZeroBL?amar_p wrote:I've been watching Trump's daily briefings for a while since there is so little high quality real time entertainment these days. Its clear that he suffers from a lot of personality disorders that would earn epithets like jerk, idiot, maniac, toxic....
One of these disorders is the compulsive need to be seen as the smartest person in the room, all the time. So he restates, paraphrases what stuff he has been able to comprehend so that he can show off to you that "he got it!", and since he considers everyone else to be dumber that himself, he'll dumb it down and explain it for you.
Endless source of entertainment with sometimes disastrous consequences.
They are the dumbest.
Trump for all his dumbness is good for India.
We should support Trump just like Porkis who supported the guileless Sardar, Bar dancer and her dumb son.
Re: Wuhan Coronavirus Resource Thread
Its a sad state of affairs in US politics right now. We have an impeached crazy monkey in power and headless chicken hoping to dislodge him in November. The level of intellectual and ideological bankruptcy across the spectrum is appalling and depressing.
While Trump may appear favourable to India, he is swayed by the last thing he has seen or heard. Highly unreliable. While India may feel they achieved some great relationship with US when Trump visted India praised Modi & India during all the show that was put up, he says pretty much the same things "wonderful", "perfect", "tremendous", "greatest ever"... to anything he does or anyone he meets.
If India's clear eyed strategy is to keep the OrangeUtan happy enough to avoid getting on to his wrong side and we hedge our bets, we might be OK. This is what I read between the lines when I hear EAM S Jaishankar speak. But if we hang our coat on Trump coming to our aid in any meaningful and long term strategic way, that would be a costly mistake.
This should be discussed in the Understaning US thread.
While Trump may appear favourable to India, he is swayed by the last thing he has seen or heard. Highly unreliable. While India may feel they achieved some great relationship with US when Trump visted India praised Modi & India during all the show that was put up, he says pretty much the same things "wonderful", "perfect", "tremendous", "greatest ever"... to anything he does or anyone he meets.
If India's clear eyed strategy is to keep the OrangeUtan happy enough to avoid getting on to his wrong side and we hedge our bets, we might be OK. This is what I read between the lines when I hear EAM S Jaishankar speak. But if we hang our coat on Trump coming to our aid in any meaningful and long term strategic way, that would be a costly mistake.
This should be discussed in the Understaning US thread.
Re: Wuhan Coronavirus Resource Thread
Seems like a light version of snake oil to me. Heck all it takes is a fiber optic cable with a UV light source at one end. I couldn't find any "in vitro" study results published by them on this "concept". The video is very dubious for a number of reasons anyone with basic physics and biology grasp will be able to point out.ldev wrote:This is what Trump was talking about, treatment developed by Cedars Sinai Hospital. Basically a UV light which is inserted down via the mouth. Now licensed to Aytu BioScience. It is claimed to kill all kinds of viruses including the coronavirus.srai wrote: Anything coming out of Trump is a “misquote”
Don’t watch his briefings for any value other than for entertainment purposes. Constantly peddling rumors, lies and partisan extremism. No substance.
Cedars-Sinai-Developed ‘Healight' Medical Device Platform Technology Being Studied as a Potential First-in-Class COVID-19 Treatment
https://streamable.com/w7rpbn
This tells us that peddlers of such unproven stuff are able to get access to the White House and the President and are able to "impress" them sufficiently to get mentioned by the President on national TV . I mean, WTF ?
Re: Wuhan Coronavirus Resource Thread
There has been a 2000 case increase since yesterday. The daily increase is trending higher but there have been 600 recoveries too. With the relaxation in lock down and ramzan, I expect there will be far more cases in the coming days. I just hope our capacity for test kits, PPE, icu, ventilators comes online by then.
Re: Wuhan Coronavirus Resource Thread
https://www.foxnews.com/us/states-spike ... trol-callsMort Walker wrote:Are you sure?srai wrote:^^^
Well, the next day he was saying what he said was in sarcasm
There is a rumour of Vicar in US having succumbed to injecting disinfectant doing rounds on twitter in UK
Re: Wuhan Coronavirus Resource Thread
There is a trial going on in India with leprosy drug. @dasgobardhan is also the first to suggest BCG vaccination will be benefecial.
Anand Ranganathan
@ARanganathan72
Early days but it appears Prof
@dasgobardhan
's suggestion is bearing fruit. PGI, Chandigarh reports improvement in critical CoVID patients upon administration of M(w) strain.
Those in power did not even thank Prof Das for his idea. But we do. THANK YOU.
Re: Wuhan Coronavirus Resource Thread
well put ...amar_p wrote:Its a sad state of affairs in US politics right now. We have an impeached crazy monkey in power and headless chicken hoping to dislodge him in November. The level of intellectual and ideological bankruptcy across the spectrum is appalling and depressing.
While Trump may appear favourable to India, he is swayed by the last thing he has seen or heard. Highly unreliable. While India may feel they achieved some great relationship with US when Trump visted India praised Modi & India during all the show that was put up, he says pretty much the same things "wonderful", "perfect", "tremendous", "greatest ever"... to anything he does or anyone he meets.
If India's clear eyed strategy is to keep the OrangeUtan happy enough to avoid getting on to his wrong side and we hedge our bets, we might be OK. This is what I read between the lines when I hear EAM S Jaishankar speak. But if we hang our coat on Trump coming to our aid in any meaningful and long term strategic way, that would be a costly mistake.
This should be discussed in the Understaning US thread.
Modi knows how to keep T happy
-
Manish_Sharma
- BRF Oldie
- Posts: 5128
- Joined: 07 Sep 2009 16:17
Re: Wuhan Coronavirus Resource Thread
Twitter
@amitabhj3156:
The Infection That’s Silently Killing Coronavirus Patients
This is what I learned during 10 days of treating Covid pneumonia at Bellevue Hospital.
By Richard Levitan
Dr. Levitan is an emergency doctor.
April 20, 2020
I have been practicing emergency medicine for 30 years. In 1994 I invented an imaging system for teaching intubation, the procedure of inserting breathing tubes. This led me to perform research into this procedure, and subsequently teach airway procedure courses to physicians worldwide for the last two decades.
So at the end of March, as a crush of Covid-19 patients began overwhelming hospitals in New York City, I volunteered to spend 10 days at Bellevue, helping at the hospital where I trained. Over those days, I realized that we are not detecting the deadly pneumonia the virus causes early enough and that we could be doing more to keep patients off ventilators — and alive.
On the long drive to New York from my home in New Hampshire, I called my friend Nick Caputo, an emergency physician in the Bronx, who was already in the thick of it. I wanted to know what I was facing, how to stay safe and what his insights into airway management with this disease were. “Rich,” he said, “it’s like nothing I’ve ever seen before.”
He was right. Pneumonia caused by the coronavirus has had a stunning impact on the city’s hospital system. Normally an E.R. has a mix of patients with conditions ranging from the serious, such as heart attacks, strokes and traumatic injuries, to the non-life-threatening, such as minor lacerations, intoxication, orthopedic injuries and migraine headaches.
During my recent time at Bellevue, though, almost all the E.R. patients had Covid pneumonia. Within the first hour of my first shift I inserted breathing tubes into two patients.
Even patients without respiratory complaints had Covid pneumonia. The patient stabbed in the shoulder, whom we X-rayed because we worried he had a collapsed lung, actually had Covid pneumonia. In patients on whom we did CT scans because they were injured in falls, we coincidentally found Covid pneumonia. Elderly patients who had passed out for unknown reasons and a number of diabetic patients were found to have it.
And here is what really surprised us: These patients did not report any sensation of breathing problems, even though their chest X-rays showed diffuse pneumonia and their oxygen was below normal. How could this be?
We are just beginning to recognize that Covid pneumonia initially causes a form of oxygen deprivation we call “silent hypoxia” — “silent” because of its insidious, hard-to-detect nature.
Pneumonia is an infection of the lungs in which the air sacs fill with fluid or pus. Normally, patients develop chest discomfort, pain with breathing and other breathing problems. But when Covid pneumonia first strikes, patients don’t feel short of breath, even as their oxygen levels fall. And by the time they do, they have alarmingly low oxygen levels and moderate-to-severe pneumonia (as seen on chest X-rays). Normal oxygen saturation for most persons at sea level is 94 to 100 percent; Covid pneumonia patients I saw had oxygen saturations as low as 50 percent.
To my amazement, most patients I saw said they had been sick for a week or so with fever, cough, upset stomach and fatigue, but they only became short of breath the day they came to the hospital. Their pneumonia had clearly been going on for days, but by the time they felt they had to go to the hospital, they were often already in critical condition.
In emergency departments we insert breathing tubes in critically ill patients for a variety of reasons. In my 30 years of practice, however, most patients requiring emergency intubation are in shock, have altered mental status or are grunting to breathe. Patients requiring intubation because of acute hypoxia are often unconscious or using every muscle they can to take a breath. They are in extreme duress. Covid pneumonia cases are very different.
A vast majority of Covid pneumonia patients I met had remarkably low oxygen saturations at triage — seemingly incompatible with life — but they were using their cellphones as we put them on monitors. Although breathing fast, they had relatively minimal apparent distress, despite dangerously low oxygen levels and terrible pneumonia on chest X-rays.
We are only just beginning to understand why this is so. The coronavirus attacks lung cells that make surfactant. This substance helps the air sacs in the lungs stay open between breaths and is critical to normal lung function. As the inflammation from Covid pneumonia starts, it causes the air sacs to collapse, and oxygen levels fall. Yet the lungs initially remain “compliant,” not yet stiff or heavy with fluid. This means patients can still expel carbon dioxide — and without a buildup of carbon dioxide, patients do not feel short of breath.
Patients compensate for the low oxygen in their blood by breathing faster and deeper — and this happens without their realizing it. This silent hypoxia, and the patient’s physiological response to it, causes even more inflammation and more air sacs to collapse, and the pneumonia worsens until oxygen levels plummet. In effect, patients are injuring their own lungs by breathing harder and harder. Twenty percent of Covid pneumonia patients then go on to a second and deadlier phase of lung injury. Fluid builds up and the lungs become stiff, carbon dioxide rises, and patients develop acute respiratory failure.
By the time patients have noticeable trouble breathing and present to the hospital with dangerously low oxygen levels, many will ultimately require a ventilator.
Silent hypoxia progressing rapidly to respiratory failure explains cases of Covid-19 patients dying suddenly after not feeling short of breath. (It appears that most Covid-19 patients experience relatively mild symptoms and get over the illness in a week or two without treatment.)
A major reason this pandemic is straining our health system is the alarming severity of lung injury patients have when they arrive in emergency rooms. Covid-19 overwhelmingly kills through the lungs. And because so many patients are not going to the hospital until their pneumonia is already well advanced, many wind up on ventilators, causing shortages of the machines. And once on ventilators, many die.
Avoiding the use of a ventilator is a huge win for both patient and the health care system. The resources needed for patients on ventilators are staggering. Vented patients require multiple sedatives so that they don’t buck the vent or accidentally remove their breathing tubes; they need intravenous and arterial lines, IV medicines and IV pumps. In addition to a tube in the trachea, they have tubes in their stomach and bladder. Teams of people are required to move each patient, turning them on their stomach and then their back, twice a day to improve lung function.
There is a way we could identify more patients who have Covid pneumonia sooner and treat them more effectively — and it would not require waiting for a coronavirus test at a hospital or doctor’s office. It requires detecting silent hypoxia early through a common medical device that can be purchased without a prescription at most pharmacies: a pulse oximeter.
Pulse oximetry is no more complicated than using a thermometer. These small devices turn on with one button and are placed on a fingertip. In a few seconds, two numbers are displayed: oxygen saturation and pulse rate. Pulse oximeters are extremely reliable in detecting oxygenation problems and elevated heart rates.
Pulse oximeters helped save the lives of two emergency physicians I know, alerting them early on to the need for treatment. When they noticed their oxygen levels declining, both went to the hospital and recovered (though one waited longer and required more treatment). Detection of hypoxia, early treatment and close monitoring apparently also worked for Boris Johnson, the British prime minister.
Widespread pulse oximetry screening for Covid pneumonia — whether people check themselves on home devices or go to clinics or doctors’ offices — could provide an early warning system for the kinds of breathing problems associated with Covid pneumonia.
People using the devices at home would want to consult with their doctors to reduce the number of people who come to the E.R. unnecessarily because they misinterpret their device. There also may be some patients who have unrecognized chronic lung problems and have borderline or slightly low oxygen saturations unrelated to Covid-19.
All patients who have tested positive for the coronavirus should have pulse oximetry monitoring for two weeks, the period during which Covid pneumonia typically develops. All persons with cough, fatigue and fevers should also have pulse oximeter monitoring even if they have not had virus testing, or even if their swab test was negative, because those tests are only about 70 percent accurate. A vast majority of Americans who have been exposed to the virus don’t know it.
There are other things we can do as well to avoid immediately resorting to intubation and a ventilator. Patient positioning maneuvers (having patients lie on their stomach and sides) open up the lower and posterior lungs most affected in Covid pneumonia. Oxygenation and positioning helped patients breathe easier and seemed to prevent progression of the disease in many cases. In a preliminary study by Dr. Caputo, this strategy helped keep three out of four patients with advanced Covid pneumonia from needing a ventilator in the first 24 hours.
To date, Covid-19 has killed more than 40,600people nationwide — more than 10,000 in New York State alone. Oximeters are not 100 percent accurate, and they are not a panacea. There will be deaths and bad outcomes that are not preventable. We don’t fully understand why certain patients get so sick, or why some go on to develop multi-organ failure. Many elderly people, already weak with chronic illness, and those with underlying lung disease do very poorly with Covid pneumonia, despite aggressive treatment.
But we can do better. Right now, many emergency rooms are either being crushed by this one disease or waiting for it to hit. We must direct resources to identifying and treating the initial phase of Covid pneumonia earlier by screening for silent hypoxia.
It’s time to get ahead of this virus instead of chasing it.
Richard Levitan, an emergency physician in Littleton, N.H., is president of Airway Cam Technologies, a company that teaches courses in intubation and airway management.
@amitabhj3156:
https://www.nytimes.com/2020/04/20/opin ... pjYNXNmAHSvia @NYTOpinion This emergency doctor says a quick and simple non-intrusive test at home - testing your oxygen saturation level - can give an early warning of the deadly #Covid_19 - and potentially save your life https://t.co/pjYNXNmAHS
The Infection That’s Silently Killing Coronavirus Patients
This is what I learned during 10 days of treating Covid pneumonia at Bellevue Hospital.
By Richard Levitan
Dr. Levitan is an emergency doctor.
April 20, 2020
I have been practicing emergency medicine for 30 years. In 1994 I invented an imaging system for teaching intubation, the procedure of inserting breathing tubes. This led me to perform research into this procedure, and subsequently teach airway procedure courses to physicians worldwide for the last two decades.
So at the end of March, as a crush of Covid-19 patients began overwhelming hospitals in New York City, I volunteered to spend 10 days at Bellevue, helping at the hospital where I trained. Over those days, I realized that we are not detecting the deadly pneumonia the virus causes early enough and that we could be doing more to keep patients off ventilators — and alive.
On the long drive to New York from my home in New Hampshire, I called my friend Nick Caputo, an emergency physician in the Bronx, who was already in the thick of it. I wanted to know what I was facing, how to stay safe and what his insights into airway management with this disease were. “Rich,” he said, “it’s like nothing I’ve ever seen before.”
He was right. Pneumonia caused by the coronavirus has had a stunning impact on the city’s hospital system. Normally an E.R. has a mix of patients with conditions ranging from the serious, such as heart attacks, strokes and traumatic injuries, to the non-life-threatening, such as minor lacerations, intoxication, orthopedic injuries and migraine headaches.
During my recent time at Bellevue, though, almost all the E.R. patients had Covid pneumonia. Within the first hour of my first shift I inserted breathing tubes into two patients.
Even patients without respiratory complaints had Covid pneumonia. The patient stabbed in the shoulder, whom we X-rayed because we worried he had a collapsed lung, actually had Covid pneumonia. In patients on whom we did CT scans because they were injured in falls, we coincidentally found Covid pneumonia. Elderly patients who had passed out for unknown reasons and a number of diabetic patients were found to have it.
And here is what really surprised us: These patients did not report any sensation of breathing problems, even though their chest X-rays showed diffuse pneumonia and their oxygen was below normal. How could this be?
We are just beginning to recognize that Covid pneumonia initially causes a form of oxygen deprivation we call “silent hypoxia” — “silent” because of its insidious, hard-to-detect nature.
Pneumonia is an infection of the lungs in which the air sacs fill with fluid or pus. Normally, patients develop chest discomfort, pain with breathing and other breathing problems. But when Covid pneumonia first strikes, patients don’t feel short of breath, even as their oxygen levels fall. And by the time they do, they have alarmingly low oxygen levels and moderate-to-severe pneumonia (as seen on chest X-rays). Normal oxygen saturation for most persons at sea level is 94 to 100 percent; Covid pneumonia patients I saw had oxygen saturations as low as 50 percent.
To my amazement, most patients I saw said they had been sick for a week or so with fever, cough, upset stomach and fatigue, but they only became short of breath the day they came to the hospital. Their pneumonia had clearly been going on for days, but by the time they felt they had to go to the hospital, they were often already in critical condition.
In emergency departments we insert breathing tubes in critically ill patients for a variety of reasons. In my 30 years of practice, however, most patients requiring emergency intubation are in shock, have altered mental status or are grunting to breathe. Patients requiring intubation because of acute hypoxia are often unconscious or using every muscle they can to take a breath. They are in extreme duress. Covid pneumonia cases are very different.
A vast majority of Covid pneumonia patients I met had remarkably low oxygen saturations at triage — seemingly incompatible with life — but they were using their cellphones as we put them on monitors. Although breathing fast, they had relatively minimal apparent distress, despite dangerously low oxygen levels and terrible pneumonia on chest X-rays.
We are only just beginning to understand why this is so. The coronavirus attacks lung cells that make surfactant. This substance helps the air sacs in the lungs stay open between breaths and is critical to normal lung function. As the inflammation from Covid pneumonia starts, it causes the air sacs to collapse, and oxygen levels fall. Yet the lungs initially remain “compliant,” not yet stiff or heavy with fluid. This means patients can still expel carbon dioxide — and without a buildup of carbon dioxide, patients do not feel short of breath.
Patients compensate for the low oxygen in their blood by breathing faster and deeper — and this happens without their realizing it. This silent hypoxia, and the patient’s physiological response to it, causes even more inflammation and more air sacs to collapse, and the pneumonia worsens until oxygen levels plummet. In effect, patients are injuring their own lungs by breathing harder and harder. Twenty percent of Covid pneumonia patients then go on to a second and deadlier phase of lung injury. Fluid builds up and the lungs become stiff, carbon dioxide rises, and patients develop acute respiratory failure.
By the time patients have noticeable trouble breathing and present to the hospital with dangerously low oxygen levels, many will ultimately require a ventilator.
Silent hypoxia progressing rapidly to respiratory failure explains cases of Covid-19 patients dying suddenly after not feeling short of breath. (It appears that most Covid-19 patients experience relatively mild symptoms and get over the illness in a week or two without treatment.)
A major reason this pandemic is straining our health system is the alarming severity of lung injury patients have when they arrive in emergency rooms. Covid-19 overwhelmingly kills through the lungs. And because so many patients are not going to the hospital until their pneumonia is already well advanced, many wind up on ventilators, causing shortages of the machines. And once on ventilators, many die.
Avoiding the use of a ventilator is a huge win for both patient and the health care system. The resources needed for patients on ventilators are staggering. Vented patients require multiple sedatives so that they don’t buck the vent or accidentally remove their breathing tubes; they need intravenous and arterial lines, IV medicines and IV pumps. In addition to a tube in the trachea, they have tubes in their stomach and bladder. Teams of people are required to move each patient, turning them on their stomach and then their back, twice a day to improve lung function.
There is a way we could identify more patients who have Covid pneumonia sooner and treat them more effectively — and it would not require waiting for a coronavirus test at a hospital or doctor’s office. It requires detecting silent hypoxia early through a common medical device that can be purchased without a prescription at most pharmacies: a pulse oximeter.
Pulse oximetry is no more complicated than using a thermometer. These small devices turn on with one button and are placed on a fingertip. In a few seconds, two numbers are displayed: oxygen saturation and pulse rate. Pulse oximeters are extremely reliable in detecting oxygenation problems and elevated heart rates.
Pulse oximeters helped save the lives of two emergency physicians I know, alerting them early on to the need for treatment. When they noticed their oxygen levels declining, both went to the hospital and recovered (though one waited longer and required more treatment). Detection of hypoxia, early treatment and close monitoring apparently also worked for Boris Johnson, the British prime minister.
Widespread pulse oximetry screening for Covid pneumonia — whether people check themselves on home devices or go to clinics or doctors’ offices — could provide an early warning system for the kinds of breathing problems associated with Covid pneumonia.
People using the devices at home would want to consult with their doctors to reduce the number of people who come to the E.R. unnecessarily because they misinterpret their device. There also may be some patients who have unrecognized chronic lung problems and have borderline or slightly low oxygen saturations unrelated to Covid-19.
All patients who have tested positive for the coronavirus should have pulse oximetry monitoring for two weeks, the period during which Covid pneumonia typically develops. All persons with cough, fatigue and fevers should also have pulse oximeter monitoring even if they have not had virus testing, or even if their swab test was negative, because those tests are only about 70 percent accurate. A vast majority of Americans who have been exposed to the virus don’t know it.
There are other things we can do as well to avoid immediately resorting to intubation and a ventilator. Patient positioning maneuvers (having patients lie on their stomach and sides) open up the lower and posterior lungs most affected in Covid pneumonia. Oxygenation and positioning helped patients breathe easier and seemed to prevent progression of the disease in many cases. In a preliminary study by Dr. Caputo, this strategy helped keep three out of four patients with advanced Covid pneumonia from needing a ventilator in the first 24 hours.
To date, Covid-19 has killed more than 40,600people nationwide — more than 10,000 in New York State alone. Oximeters are not 100 percent accurate, and they are not a panacea. There will be deaths and bad outcomes that are not preventable. We don’t fully understand why certain patients get so sick, or why some go on to develop multi-organ failure. Many elderly people, already weak with chronic illness, and those with underlying lung disease do very poorly with Covid pneumonia, despite aggressive treatment.
But we can do better. Right now, many emergency rooms are either being crushed by this one disease or waiting for it to hit. We must direct resources to identifying and treating the initial phase of Covid pneumonia earlier by screening for silent hypoxia.
It’s time to get ahead of this virus instead of chasing it.
Richard Levitan, an emergency physician in Littleton, N.H., is president of Airway Cam Technologies, a company that teaches courses in intubation and airway management.
Re: Wuhan Coronavirus Resource Thread
How does this square with the news reports that in India use of ventilators is very minimal. More patients die of multiple organ failure than due to pnemonia as the case seems to be in Wuhan virus patients in US?
Re: Wuhan Coronavirus Resource Thread
Huge list of items - despite a lot of derivative kit, to develop all this in 2-3 months, and rush it to production in a lockdown, is a big deal.
Critical Equipment and Technologies Developed by DRDO for Combating COVID19 Pandemic 20/04/2020
https://drdo.gov.in/sites/default/files ... ttach2.pdf
An expanded list
https://www.drdo.gov.in/message-board/d ... t-covid-19
Critical Equipment and Technologies Developed by DRDO for Combating COVID19 Pandemic 20/04/2020
https://drdo.gov.in/sites/default/files ... ttach2.pdf
An expanded list
https://www.drdo.gov.in/message-board/d ... t-covid-19
Re: Wuhan Coronavirus Resource Thread
The worldometer/info website for new cases in the US (and world) seems really funky and wonky. I looked up the number of new cases today for *yesterday* i.e. 24 hours ago mid-night GMT, And that was at 10,000+ !!. And the guvnor of NY (Cuomo) his press conference today indicates there were 1000 new cases. worldometer/info showed 4500 cases 3 days ago and steadily increased to 10,000 today (for yesterday). Something seriously off.
By the way, Cuomo's press conferences are informative, precise and reasonable. THey are discussing how to open NY state (= NY city and rest of New York). The back-and-forth on the questions shows he has a grasp of what's going on, where things are clear, and where they are not (known unknowns and unknown unknowns). He sez dat widespead antibody testing and Covid infection testing will be core to re-opening the state and economy. Which makes sense. Otherwise you wont know if a major drop in new cases for a month is real or is it a false dawn. This may be applicable to beyond NY state, possibly India.
By the way, Cuomo's press conferences are informative, precise and reasonable. THey are discussing how to open NY state (= NY city and rest of New York). The back-and-forth on the questions shows he has a grasp of what's going on, where things are clear, and where they are not (known unknowns and unknown unknowns). He sez dat widespead antibody testing and Covid infection testing will be core to re-opening the state and economy. Which makes sense. Otherwise you wont know if a major drop in new cases for a month is real or is it a false dawn. This may be applicable to beyond NY state, possibly India.
Re: Wuhan Coronavirus Resource Thread
OK, so somebody else noticed besides me. More than case count, the US death count has been seriously modified. I was doing a comparison with the official prediction of 93,000 deaths by Aug. 1, which also had a daily breakdown. Up to Apr. 13, I was noticing a trend where the actual deaths were starting to fall well below the predictions, and I was confident that the final count would be less than half the prediction. Then on Apr. 14, there was a new criterion for counting deaths (just in NY state, or whole US? Don't know). Suddenly on Apr. 15, the daily death count shot up to 4X what it was on Apr. 13. On the plot, it was a huge outlier. I don't know what they did after that, probably redistributed those deaths to smoothen the curve back. But since Apr. 15, the "actual" US cumulative death count has gone right back to the 93,000 prediction.SriKumar wrote:The worldometer/info website for new cases in the US (and world) seems really funky and wonky. I looked up the number of new cases today for *yesterday* i.e. 24 hours ago mid-night GMT, And that was at 10,000+ !!. And the guvnor of NY (Cuomo) his press conference today indicates there were 1000 new cases. worldometer/info showed 4500 cases 3 days ago and steadily increased to 10,000 today (for yesterday). Something seriously off.
By the way, Cuomo's press conferences are informative, precise and reasonable. THey are discussing how to open NY state (= NY city and rest of New York). The back-and-forth on the questions shows he has a grasp of what's going on, where things are clear, and where they are not (known unknowns and unknown unknowns). He sez dat widespead antibody testing and Covid infection testing will be core to re-opening the state and economy. Which makes sense. Otherwise you wont know if a major drop in new cases for a month is real or is it a false dawn. This may be applicable to beyond NY state, possibly India.
Just to point out - the prediction came from training a data model using data up to about the beginning of April, using actual numbers. Those actual numbers followed the old criterion, whatever that was. And the model was seriously overpredicting according to that criterion. With the new criterion for counting deaths, the prediction seems right on the dot, but this is deceptive, because the prediction was based on training data from the old criterion. It's like taking the yearly car sales figures in the US, training a model based on that, using the model to predict future car sales, then suddenly changing the criterion to count both cars and commercial trucks, but still using the old model to make predictions. This is a pretty exact analogy for what seems to have happened. So I gave up on the comparison.
So it seems the US is still going to have about 90,000 deaths by Aug. 1st. If the model had been properly trained using the new criterion for counting deaths from the beginning, then the model would have predicted about twice this figure - 180,000 deaths. Just pointing out that data modeling is all very fine, but they got the numbers wrong. It seems on this thread the attitude is "what do you know about it, and why are you questioning the experts?" Not questioning the experts, just maintaining my own independent thinking and doing post verification, that's all. I'm scrupulously following the guidelines they laid down, but at the end of it all, I want to know how much they actually knew the whole time.
In fact, that model also predicted usage of hospital beds, ICU beds, and ventilators, and there was somebody who pulled actual numbers on these, which pointed out that as of April 5th, the model had overestimated hospital bed use by 8X, ICU bed usage by 6.4X, and ventilator usage by 40X. And the model also fully accounted for the lockdown.
-
DrRatnadip
- BRFite
- Posts: 604
- Joined: 31 Dec 2016 00:40
Re: Wuhan Coronavirus Resource Thread
Mumbai: 36-year-old doctor dies of multiple organ failure, samples test positive for Covid-19 - India Today | DailyHunt Lite
http://dhunt.in/9o2f3?ss=wsp&s=wa
A 36-year-old general physician, who consulted at two private hospitals in Mumbai's Govandi, succumbed to the novel coronavirus infection on Thursday. He is likely to have contracted the virus from a patient at the hospital.
The doctor did not have any co-morbid conditions and died of Acute Respiratory Distress Syndrome due to Covid-19 along with multiple organ failure. He was declared dead at around 1:55 am on Thursday at SL Raheja Hospital. The doctor started showing symptoms such as loose motions and breathlessness on April 13.
He was admitted to the Sion Hospital in the wee hours of April 15 where he was tested for Covid-19. As his condition was deteriorating and an ICU bed was not available at Sion, he was shifted to Somaiya Hospital in Vidyavihar.
At Somaiya hospital, his breathing improved but he needed dialysis.
As he was a suspected Covid-19 patient, Somaiya hospital administration said that he will have to be shifted to Raheja hospital as they have dialysis for Covid-19 patients.
"My brother had to be shifted on oxygen to Raheja and no cardiac ambulance was ready to transport a Covid-19 patient. He was on a ventilator. After looking at his deteriorating condition, we shifted him using a normal ambulance. His samples have returned positive for Covid-19," said the deceased's brother who is also a doctor.
The doctor's condition kept deteriorating. He had a multi-organ failure with deranged liver function test, acute renal failure and bleeding disorder. His condition further worsened on Wednesday night. Despite multiple efforts of resuscitation, he could not survive and was declared dead.
"We did not get a chance to speak with him to understand how he contracted the virus. Before going to Sion, we tried to get a bed at Kasturba hospital, but we were told no beds are available," the doctor's brother added.
"This is something we need to be very careful about. If healthcare workers are infected like this, we should be able to provide them with the best of care" said Epidemiologist Dr Om Shrivastava.
http://dhunt.in/9o2f3?ss=wsp&s=wa
A 36-year-old general physician, who consulted at two private hospitals in Mumbai's Govandi, succumbed to the novel coronavirus infection on Thursday. He is likely to have contracted the virus from a patient at the hospital.
The doctor did not have any co-morbid conditions and died of Acute Respiratory Distress Syndrome due to Covid-19 along with multiple organ failure. He was declared dead at around 1:55 am on Thursday at SL Raheja Hospital. The doctor started showing symptoms such as loose motions and breathlessness on April 13.
He was admitted to the Sion Hospital in the wee hours of April 15 where he was tested for Covid-19. As his condition was deteriorating and an ICU bed was not available at Sion, he was shifted to Somaiya Hospital in Vidyavihar.
At Somaiya hospital, his breathing improved but he needed dialysis.
As he was a suspected Covid-19 patient, Somaiya hospital administration said that he will have to be shifted to Raheja hospital as they have dialysis for Covid-19 patients.
"My brother had to be shifted on oxygen to Raheja and no cardiac ambulance was ready to transport a Covid-19 patient. He was on a ventilator. After looking at his deteriorating condition, we shifted him using a normal ambulance. His samples have returned positive for Covid-19," said the deceased's brother who is also a doctor.
The doctor's condition kept deteriorating. He had a multi-organ failure with deranged liver function test, acute renal failure and bleeding disorder. His condition further worsened on Wednesday night. Despite multiple efforts of resuscitation, he could not survive and was declared dead.
"We did not get a chance to speak with him to understand how he contracted the virus. Before going to Sion, we tried to get a bed at Kasturba hospital, but we were told no beds are available," the doctor's brother added.
"This is something we need to be very careful about. If healthcare workers are infected like this, we should be able to provide them with the best of care" said Epidemiologist Dr Om Shrivastava.
Re: Wuhan Coronavirus Resource Thread
Deleted.
Try the Korea thread.
Try the Korea thread.
Re: Wuhan Coronavirus Resource Thread
Do Lockdowns Save Many Lives? In Most Places, the Data Say No
We ran a simple one-variable correlation of deaths per million and days to shutdown, which ranged from minus-10 days (some states shut down before any sign of Covid-19) to 35 days for South Dakota, one of seven states with limited or no shutdown. The correlation coefficient was 5.5%—so low that the engineers I used to employ would have summarized it as “no correlation” and moved on to find the real cause of the problem.
No conclusions can be drawn about the states that sheltered quickly, because their death rates ran the full gamut, from 20 per million in Oregon to 360 in New York. This wide variation means that other variables—like population density or subway use—were more important. Our correlation coefficient for per-capita death rates vs. the population density was 44%.
Re: Wuhan Coronavirus Resource Thread
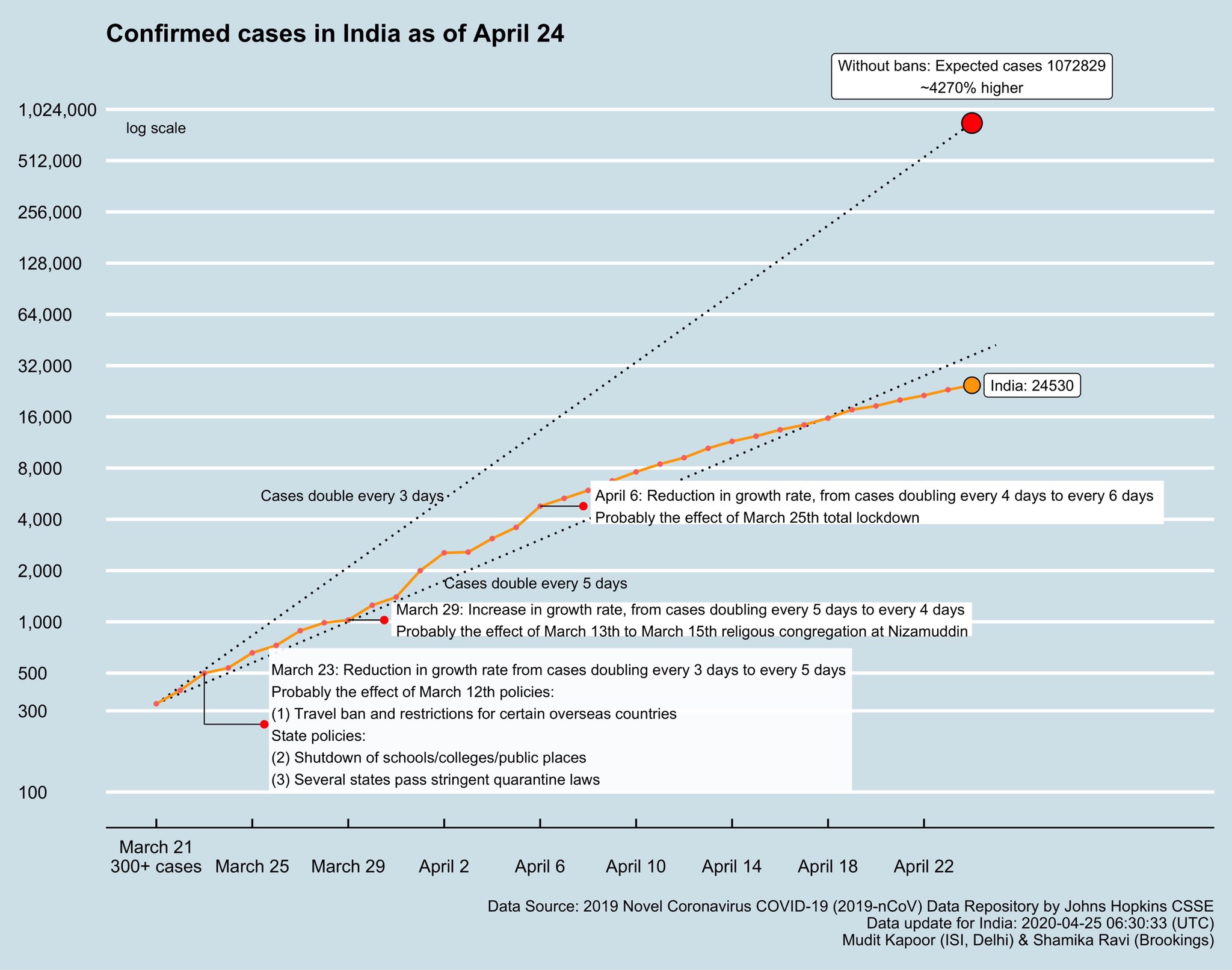
23 April 2020 - 500542
24 April 2020 - 541789
25 April 2020 - 579957
26 April 2020 - 625309
27 April 2020 - 665819
According to covid19india.org, 1607 confirmed cases were reported yesterday (26th).
-
Mort Walker
- BRF Oldie
- Posts: 10040
- Joined: 31 May 2004 11:31
- Location: The rings around Uranus.
Re: Wuhan Coronavirus Resource Thread
NY State was under reporting deaths in nursing homes that were suspected to be COVID-19. There was a note about it some days back in the WSJ. It is likely that both NY and CA are under reporting deaths for political reasons.SriKumar wrote:The worldometer/info website for new cases in the US (and world) seems really funky and wonky. I looked up the number of new cases today for *yesterday* i.e. 24 hours ago mid-night GMT, And that was at 10,000+ !!. And the guvnor of NY (Cuomo) his press conference today indicates there were 1000 new cases. worldometer/info showed 4500 cases 3 days ago and steadily increased to 10,000 today (for yesterday). Something seriously off.
By the way, Cuomo's press conferences are informative, precise and reasonable. THey are discussing how to open NY state (= NY city and rest of New York). The back-and-forth on the questions shows he has a grasp of what's going on, where things are clear, and where they are not (known unknowns and unknown unknowns). He sez dat widespead antibody testing and Covid infection testing will be core to re-opening the state and economy. Which makes sense. Otherwise you wont know if a major drop in new cases for a month is real or is it a false dawn. This may be applicable to beyond NY state, possibly India.
Re: Wuhan Coronavirus Resource Thread
Pune's Serum Institute to start making coronavirus vaccine that is under trial
3 min read . Updated: 26 Apr 2020, 02:17 PM IST
* Serum Institute of India will be manufacturing Oxford University's coronavirus vaccine in anticipation of clinical trials succeeding by September-October in the UK
* The company expressed optimism of starting trials in India for this vaccine over the next 2-3 weeks
SII has collaborated with scientists at Oxford University for a malaria vaccine project in the past and can say with certainty that they are some of the best scientists, he added.
"We expect the (COVID-19) vaccine to be out in the market by September - October, only if the trials are successful with the requisite safety and assured efficacy. We will be starting trials in India for this vaccine hopefully over the next 2-3 weeks' time," Poonawalla said.
"Following that, we have undertaken the decision to initiate manufacturing at our own risk. The decision has been solely taken to have a jump-start on manufacturing, to have enough doses available, if the clinical trials prove successful," Poonawalla said.
The company plans to initiate the trials in India for the vaccine with necessary regulatory approvals, which are underway presently.
"Keeping the current situation in mind, we have funded this endeavour at a personal capacity and hopefully will be able to enlist the support of other partners to further scale-up the vaccine production," Poonawalla said.
The vaccines will be manufactured at the company's facility in Pune. Building a new facility for COVID-19 vaccine would have taken around 2-3 years, he added.
https://www.livemint.com/news/india/pun ... 21799.html
3 min read . Updated: 26 Apr 2020, 02:17 PM IST
* Serum Institute of India will be manufacturing Oxford University's coronavirus vaccine in anticipation of clinical trials succeeding by September-October in the UK
* The company expressed optimism of starting trials in India for this vaccine over the next 2-3 weeks
SII has collaborated with scientists at Oxford University for a malaria vaccine project in the past and can say with certainty that they are some of the best scientists, he added.
"We expect the (COVID-19) vaccine to be out in the market by September - October, only if the trials are successful with the requisite safety and assured efficacy. We will be starting trials in India for this vaccine hopefully over the next 2-3 weeks' time," Poonawalla said.
"Following that, we have undertaken the decision to initiate manufacturing at our own risk. The decision has been solely taken to have a jump-start on manufacturing, to have enough doses available, if the clinical trials prove successful," Poonawalla said.
The company plans to initiate the trials in India for the vaccine with necessary regulatory approvals, which are underway presently.
"Keeping the current situation in mind, we have funded this endeavour at a personal capacity and hopefully will be able to enlist the support of other partners to further scale-up the vaccine production," Poonawalla said.
The vaccines will be manufactured at the company's facility in Pune. Building a new facility for COVID-19 vaccine would have taken around 2-3 years, he added.
https://www.livemint.com/news/india/pun ... 21799.html
Re: Wuhan Coronavirus Resource Thread
With over 70% covid19 positive cases being asymptomatic as per ICMR, the real peak will happen after monsoon.
Re: Wuhan Coronavirus Resource Thread
Twitter
Malini Aisola @malini_aisola· 15h
(Co-convenor of All India Drug Action Network (AIDAN); Campaign for Dignified and Affordable Healthcare; Hip Implant Patients Support group (HIPS)
https://twitter.com/malini_aisola/statu ... 2908999680
Malini Aisola @malini_aisola· 15h
(Co-convenor of All India Drug Action Network (AIDAN); Campaign for Dignified and Affordable Healthcare; Hip Implant Patients Support group (HIPS)
1/N
Delhi High Court judgement in Rare Metabolics v Matrix Labs has revealed scandalous details about the import of 5 lac Wondfo antibody test kits, ordered by @ICMRDELHI at Rs 30cr through intermediaries who were taking a cut of 18.75 cr @CDSCO_INDIA_INF @MoHFW_INDIA @NITIAayog
2//N
Breakdown of pricing for 5 lac test kits ordered by ICMR:
Matrix import @ Rs 245 a piece = Rs 12 cr 25 lac
Matrix sale to Rare Metabolics with 7.75 cr markup = Rs. 21 cr
Rare Metabolic sale to @ICMR @ Rs 600 a piece (9cr markup)= Rs. 30 cr
3/N
Matrix is also due to provide Govt of Tamil Nadu 50k test kits through a dealer, Shan Biotech & Diagnostics and Diagnostics, at the "ICMR approved rate of @Rs.600/- per test" Due to the legal dispute b/w Rare Metabolics & Matrix, dirty details about costs have poured out.
4/N
DHC stepped in to cap price of test kits at Rs 400 inclusive of GST, noting that:
"The Court is of the view that a profit mark-up of Rs. 155/- i.e 61% on the landed cost price of Rs. 245/- is much on the higher side and in any case more than sufficient for the seller,..."
5/N
"...for the kits/tests to be made available in India for urgent extensive tests through the country, especially in these
present extraordinary circumstances of the worldwide pandemic."
6/N
However, the Rs. 400 cap may not apply to current order of 5 lac kits
Reference para 7 of judgement where Court has instructed that balance amount due to Matrix (as per the old agreed rate) should be cleared by Rare Metabolic.
7/N
The Court, apparently unaware of the quality concerns relating to these test kits & therefore ICMR's reluctance to pay Rare Metabolics, directed that, from the new consignment
- 2.24 lac kits (pending) shall be delivered to ICMR
- pending kits also be supplied to Tamil Nadu
N/N
It's hard to imagine that
@ICMRDELHI
was unaware of the profiteering by intermediaries. It would have known Wondfo price of $3/kit, prices of kits from other manufacturers & also prices at which they are being procured
Chhattisgarh has procured at ~Rs 400
@TS_SinghDeo
@ICMRDELHI
placed its order with mystery Petitioner 2 (unnamed in the order)
An agreement was signed in which Rare Metabolics appointed petitioner no.2 as its distributor for COVID 19 Rapid Test Kits & other related material to which the respondent (Matrix) also was a signatory
https://twitter.com/malini_aisola/statu ... 2908999680
Last edited by Mollick.R on 27 Apr 2020 14:09, edited 1 time in total.