Re: Wuhan Coronavirus Resource Thread
Posted: 22 Apr 2020 12:22
Shaun, Thanks.
Consortium of Indian Defence Websites
https://forums.bharat-rakshak.com/
17,000 Total17,000+ COVID cases in India as of 19 April. Only 166 needed critical care. The rest recovering with basic care.
Out of those 166, ICU needed for 87, extra oxygen needed for 55 and ventilators needed for just 24.
Only 0.14% of Corona positive cases needing ventilators at once!
A five-member Central team has projected that the number of COVID-19 cases in Mumbai will touch an estimated 42,604 by April 30 and spiral to 6,56,407 by May 15.
Based on mathematical modelling for Mumbai by the Union Ministry of Health on April 16, the data presented by the team caught the Maharastra government off guard. The State government contested the methodology and tools used for the latest projection and gap analysis.
According to the data projections initially put together by the Union Ministry of Health and Family Welfare, Mumbai’s health infrastructure during this peak would have a staggering shortage of 13,636 ventilators and 4,83,000 isolation beds.
The State government on Tuesday made a detailed presentation of its own to the visiting Inter-Ministerial Central Teams (IMCTs), highlighting the “discrepancies” in the modelling.
According to the projections presented on April 16, the shortage of isolation beds without oxygen support will touch 30,481 by April 30 in Mumbai, while beds with oxygen support will fall short by 5,466. As cases cross 40,000, the city will need another 1,200 ICU beds and 392 ventilators. When the case count touches 6,56,407 on May 15, the shortage of isolation beds without oxygen support will be a staggering 4,83,385, and shortage of ICU beds will be 27,688 while the shortage of ventilators will be 13,636, said the report, a copy of which is with The Hindu.
There are more than 50 people dying every day. So are they dying with using a ventilator? I thought all critical patients needed ventilators.pankajs wrote:https://twitter.com/KiranKS/status/125265811328441139417,000 Total17,000+ COVID cases in India as of 19 April. Only 166 needed critical care. The rest recovering with basic care.
Out of those 166, ICU needed for 87, extra oxygen needed for 55 and ventilators needed for just 24.
Only 0.14% of Corona positive cases needing ventilators at once!
166 Critical care
87 ICU
55 Oxygen
24 Ventilator
hanumadu wrote: There are more than 50 people dying every day. So are they dying with using a ventilator? I thought all critical patients needed ventilators.
The problem with this stat is what about the 500 odd deaths ? Shouldn't those be counted as serious cases as well ?pankajs wrote:https://twitter.com/KiranKS/status/125265811328441139417,000 Total17,000+ COVID cases in India as of 19 April. Only 166 needed critical care. The rest recovering with basic care.
Out of those 166, ICU needed for 87, extra oxygen needed for 55 and ventilators needed for just 24.
Only 0.14% of Corona positive cases needing ventilators at once!
166 Critical care
87 ICU
55 Oxygen
24 Ventilator
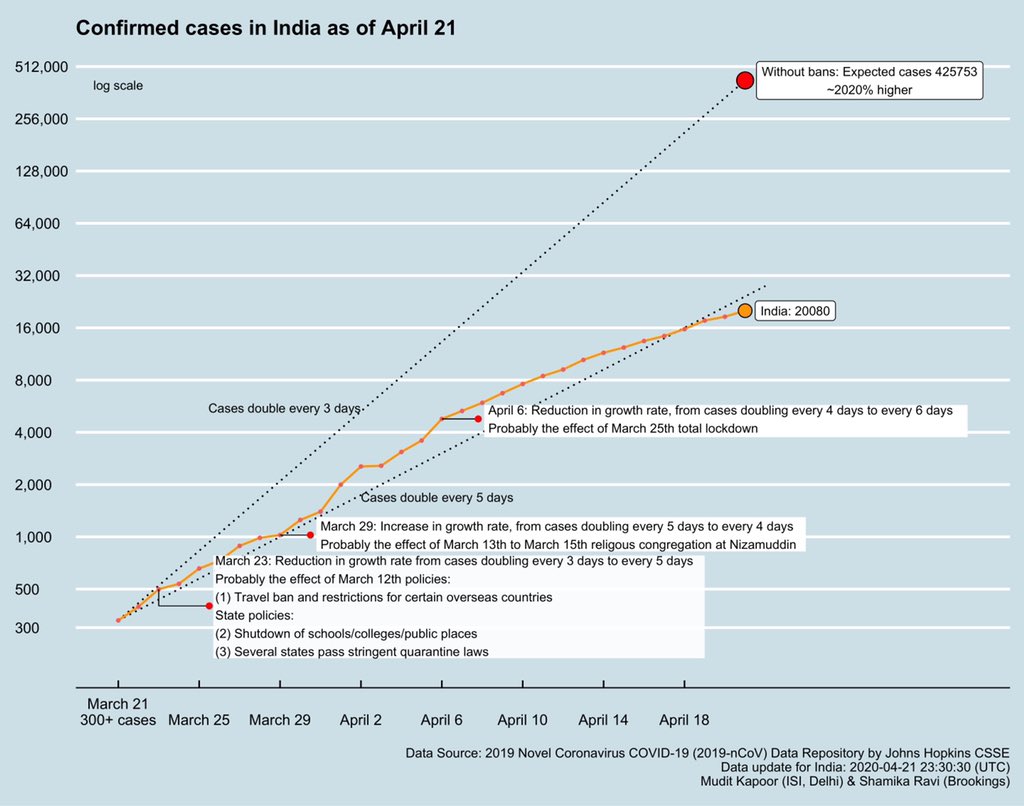
Prof Shamika Ravi @ShamikaRavi
#DailyUpdate #Covid19India
As total Confirmed cases grow in India, Active cases are growing at 6.8% - so doubling every 10 days.
We had severe shortage of ventilators even before covid pandemic.. Now significant proportion of available ventilators are diverted in Covid ICU.. This is making other routine patients requiring venti suffer..Bart S wrote:hanumadu wrote: There are more than 50 people dying every day. So are they dying with using a ventilator? I thought all critical patients needed ventilators.
That was what people initially thought, hence the hype about ventilator shortage and everybody trying to manufacture one. But it looks like the virus causes multi-organ failure and that might be what people are actually dying from, even before their lungs give way.
Comorbidities? Death per 10k is lower in California than in NY/NJ or Chicago. Generally CA has healthier lifestyle.DrRatnadip wrote: It seems average age of patients dying is lower in INDIA than in europe/ US.. Dont know cause
I will think I am taking HCQ.Mort Walker wrote:disha wrote:It's the second section in the news link which wants me to go to Gujarat & wish to be asymptomatic!
https://ahmedabadmirror.indiatimes.com/ ... 281418.cms
You do know that Guj is a dry state?
I am unsure.. Hope we are not loosing salvagable patients in govt setups.. Need to utilize private sector in better way..disha wrote:Comorbidities? Death per 10k is lower in California than in NY/NJ or Chicago. Generally CA has healthier lifestyle.DrRatnadip wrote: It seems average age of patients dying is lower in INDIA than in europe/ US.. Dont know cause
Residual Chlorine is present in most disinfected drinking-water at concentrations of 0.2–1 mg/litre( provided suitable arrangement is used for dosing sodium or calcium hypochlorite ) , can it eradicate the problem in potable water ??amar_p wrote:There are now reports of traces of Corona virus being detected in non-drinking water sources in Paris region in France. 4 out of 27 samples recently tested showed traces of virus presence. This water is mostly used for cleaning public spaces and gardening.
Water contamination is perhaps inevitable given several medical reports confirm that faecal-oral transmission is possible when an infected person does viral shedding.
Though no one currently knows at what viral concentration water thus contaminated may lead to disease spread, this is a point of alert to to public water supplies across the world, and especially to Indian local authorities given our water woes which are worst during summer and our disparate sanitation levels.
We might want to advise Aam Mamata to drink boiled & cooled water and not stored water even if it comes from a clean source. Bottled packaged water in India is sometimes dubious or spurious.
Ha - nothing of the sort, despite the friendly cow ads. Cali (the state) has lower pop density than NYC/Chicago do. Nothing at all to do with the perceived healthier lifestyle which is honestly a baseless claim.disha wrote:Comorbidities? Death per 10k is lower in California than in NY/NJ or Chicago. Generally CA has healthier lifestyle.DrRatnadip wrote: It seems average age of patients dying is lower in INDIA than in europe/ US.. Dont know cause
Calif is one of the healthier states in the country along with Hawaii and Colorado iirc. Think in terms of obesity and related diseases.Raveen wrote:Ha - nothing of the sort, despite the friendly cow ads. Cali (the state) has lower pop density than NYC/Chicago do. Nothing at all to do with the perceived healthier lifestyle which is honestly a baseless claim.disha wrote:
Comorbidities? Death per 10k is lower in California than in NY/NJ or Chicago. Generally CA has healthier lifestyle.
Aarvee Ji, it is indeed sad that a pure science person has to change his career path to make a better life. That has been the situation in the West particularly, if you want to be a doctor/lawyer/engineer, you pay through the nose for a college education, a PhD in science - you get in free. However, not much of a career opportunity after that.Aarvee wrote:It sure is saar, problem is, funding is always an issue. Some morbid humour- Pandemics like this are good for researchers, funding is assured for a few years. Other wise, there simply arent enough jobs and what ever are available, have low pay and job security.pgbhat wrote: Saar, great field. Great to have your inputs on this.
For example,
https://www.nbcnews.com/health/health-c ... d-n1150091
I too moved onto Cancer genomics as there is more money and opportunities.
chola wrote:Hmmm, I am living perfectly well in the cold environs of the Amreekan northeast. And I am full-blooded Tamil.nam wrote:Ethnic groups are dying & in ICU at a higher percentage compared to White population, in US & UK.
33% of ICU patients are ethnic, for a population of 13-14% in UK!
No yet, fully detailed study as to why, however along with cultural & dietary differences, potentially lack of Vitamin D production, which helps the immune system.
A good video by the doc.
Fundamentally we Indians are not made to live in colder place, with no sun
The high rate of ICU patients are mainly blacks and Hispanics I imagine. I don't know about the Pakis and Bangladeshis but desis in my circle seem to have a lower rate of infection than whites and I have no heard of anyone in an ICU (yet.) We seem to be far more careful and conscientious about keeping ourselves and our families safe than goras. (We use a lot of delivery for grocery instead of going out on our own, for example.) Economic class might have to do with it also. Again, those desi cab drivers (mainly pakis/other peacefuls) and convenient store clerks might be having it worse.
Obesity numbers, sure, but are you trying to tie obesity to Covid? If not, then broad statements like one state is healthier are pointless. They are "healthier" based on your chosen metric, I bet L.A. folks have more respiratory issues than someone in Wyoming thanks to that SMOG, does that make Cali less healthy?Cain Marko wrote:Calif is one of the healthier states in the country along with Hawaii and Colorado iirc. Think in terms of obesity and related diseases.Raveen wrote:
Ha - nothing of the sort, despite the friendly cow ads. Cali (the state) has lower pop density than NYC/Chicago do. Nothing at all to do with the perceived healthier lifestyle which is honestly a baseless claim.
Is that why there are trace amounts of fecal matter on every Indian Rupee note?Primus wrote:. We are as a culture more conscious of personal hygiene etc though
Eh, where is the evidence for that ? Did his words hurt you that much that you have to come up with this nonsense ?Raveen wrote:Is that why there are trace amounts of fecal matter on every Indian Rupee note?Primus wrote:. We are as a culture more conscious of personal hygiene etc though
Population density or lack of it shows up in R0 or transmission. Or rather in a given unit of time, x units will be infected vs. y units infected.Raveen wrote:Obesity numbers, sure, but are you trying to tie obesity to Covid? If not, then broad statements like one state is healthier are pointless. They are "healthier" based on your chosen metric, I bet L.A. folks have more respiratory issues than someone in Wyoming thanks to that SMOG, does that make Cali less healthy?
When you talk about infection rates per 10,000 then you are talking about R0. If COVID had any direct relationship to obesity, OK would be the worst hit state.disha wrote:Population density or lack of it shows up in R0 or transmission. Or rather in a given unit of time, x units will be infected vs. y units infected.Raveen wrote:Obesity numbers, sure, but are you trying to tie obesity to Covid? If not, then broad statements like one state is healthier are pointless. They are "healthier" based on your chosen metric, I bet L.A. folks have more respiratory issues than someone in Wyoming thanks to that SMOG, does that make Cali less healthy?
However, once they are infected the death rates are to be compared. It helps to compare death rate even state wise and county wise.
Using that, it has been found that african-americans and latinos are more likely to have a higher death rate compared to others. Is it Vitamin D deficiency? Access to health care? Co-morbities due to obesity (hypertension and diabetes)? Or simply poverty?
Poverty is a major cause of obesity in US.
Yes, CA is healthier compared to NY and NJ and yes obesity is a morbity that needs to be checked. https://www.americashealthrankings.org/ ... n/state/CA
https://pdfs.semanticscholar.org/b3b5/d ... 57534d.pdfRony wrote:Eh, where is the evidence for that ? Did his words hurt you that much that you have to come up with this nonsense ?Raveen wrote:
Is that why there are trace amounts of fecal matter on every Indian Rupee note?
Obesity is a risk factor for mortality as well as obesity related illnesses (e.g. diabetes, hypertension, coronary artery disease, etc.) but not infection as far as I'm aware of.Raveen wrote:When you talk about infection rates per 10,000 then you are talking about R0. If COVID had any direct relationship to obesity, OK would be the worst hit state.disha wrote:
Population density or lack of it shows up in R0 or transmission. Or rather in a given unit of time, x units will be infected vs. y units infected.
However, once they are infected the death rates are to be compared. It helps to compare death rate even state wise and county wise.
Using that, it has been found that african-americans and latinos are more likely to have a higher death rate compared to others. Is it Vitamin D deficiency? Access to health care? Co-morbities due to obesity (hypertension and diabetes)? Or simply poverty?
Poverty is a major cause of obesity in US.
Yes, CA is healthier compared to NY and NJ and yes obesity is a morbity that needs to be checked. https://www.americashealthrankings.org/ ... n/state/CA
Agree 100% that's my point tooDavidD wrote:Obesity is a risk factor for mortality as well as obesity related illnesses (e.g. diabetes, hypertension, coronary artery disease, etc.) but not infection as far as I'm aware of.Raveen wrote:
When you talk about infection rates per 10,000 then you are talking about R0. If COVID had any direct relationship to obesity, OK would be the worst hit state.
Very true sir. Truth be told, I seriously considered graduate entry into medicine for an MD after both masters and PhD. But got a family to look after, so cant do at this stage in life. Any way, OT for this thread so I'll stop.Primus wrote: Aarvee Ji, it is indeed sad that a pure science person has to change his career path to make a better life. That has been the situation in the West particularly, if you want to be a doctor/lawyer/engineer, you pay through the nose for a college education, a PhD in science - you get in free. However, not much of a career opportunity after that.
Wasn't there a woman holding up a sign somewhere saying something like - "You pay a biologist $1800 per month, but want a vaccine developed, why don't you ask Ronaldo to do it for you?"
That is an amazing preparation! Given the symptomatic cases are at 20k, the above capacity hopefully is not utilized.Rishi_Tri wrote:Details about India China Virus preparation shared by Prakash Javdekar yesterday:
Isolation Beds available 200,000
ICU Beds available 24,000
Ventilators available 13,000
PPE ordered with 77 manufacturers 18,800,000
N95 masks available 2,500,000
N95 masks ordered 25,000,000
Source of Information: All India Radio news
Raveen'ji, I think you have totally twisted my argument. I never ever said "COVID has direct relationship to obesity".Raveen wrote: When you talk about infection rates per 10,000 then you are talking about R0. If COVID had any direct relationship to obesity, OK would be the worst hit state.
Investigational chimp adenovirus MERS-CoV vaccine protects monkeysAs the world’s largest vaccine manufacturer, nobody ever dreamt that we do more than Glaxo or Merck or Sanofi. And they are a clutch of 20 companies or ten companies that have been merged, whereas we are a company that started as a small scale company without any government support. And, that I would consider would be a major milestone in my career, at the cost of huge profits that we have sacrificed by keeping the prices very affordable, the lowest in the world.
An investigational vaccine called ChAdOx1 MERS protected two groups of rhesus macaques from disease caused by Middle East respiratory syndrome coronavirus (MERS-CoV). The scientists’ MERS-CoV macaque study follows earlier studies of the experimental vaccine in mice. They also have successfully tested the vaccine platform against Nipah virus in hamsters and against Lassa virus in guinea pigs; they next plan to expedite testing a vaccine candidate against SARS-CoV-2. The MERS vaccine is being studied in Phase 1 human clinical trials in the United Kingdom and Saudi Arabia. The same chimpanzee adenovirus vaccine platform also is being assessed for malaria, HIV, influenza, hepatitis C, tuberculosis and Ebola.
I hope Serum is able to produce this in sufficient quantity so that India becomes the global hub for the vaccine.Gerard wrote:Our vaccine's clinical trial will start from tomorrow: Vaccinologist Adrian Hill
Production of Oxford University's ChAdOx1 nCoV-19 vaccine has already started at one partner, Serum Institute of India, the world's largest producer of vaccines. 5 million doses a month in two weeks time rising to ten million a month within six months time. Vaccine is an attenuated Chimpanzee Adenovirus capable of producing the spike (S) protein of SARS-CoV-2.
Interview with Oxford Professor Adrian Hill and Adar Poonawalla of Serum.
How is that different or worse from these in the so called first world ?Raveen wrote:https://pdfs.semanticscholar.org/b3b5/d ... 57534d.pdfRony wrote:
Eh, where is the evidence for that ? Did his words hurt you that much that you have to come up with this nonsense ?
Search
So you did not even know what his assertion is and assuming things ? I will let him speak for himself but i did not see the word *most conscious* in his assertion. He used the words * we are as a culture more conscious of personal hygiene*Raveen wrote:Also, where is the evidence to support we are the most health conscious society in the world or whatever the assertion was from OP
By the way there is feces in the swimming pools too. Hope you don't get into a swimming pool.